uMMA test
SKU:
$169.95
$169.95
$169.95
per item
NOTE: The above price reflects shipping and handling to addresses inside the contiguous (lower 48 adjoining states plus Washington, D.C.) of the U.S.A.
Additional shipping fees apply to Hawaii, Alaska, off shore American territories and possessions and to International orders.
uMMA test:
The uMMA test will reveal if the tissue is using B12. The uMMA test is noninvasive (it is a simple urinalysis) and is a much more discrete test than a serum MMA.
The uMMA test is a functional assay. uMMA reflects cobalamin (Vitamin B12) activity at the tissue/cellular level since MMA levels are directly related to a B12-dependent metabolic pathway.
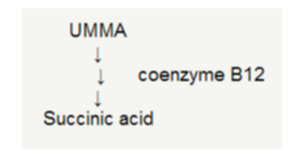
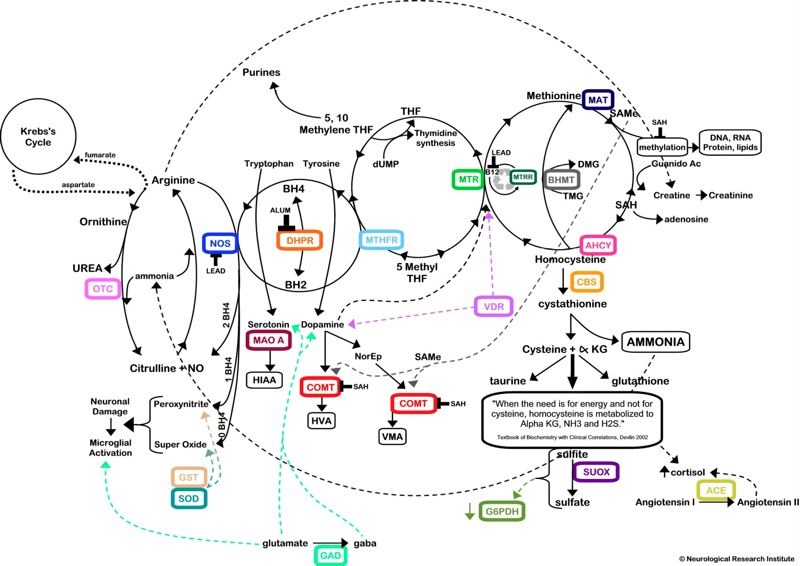
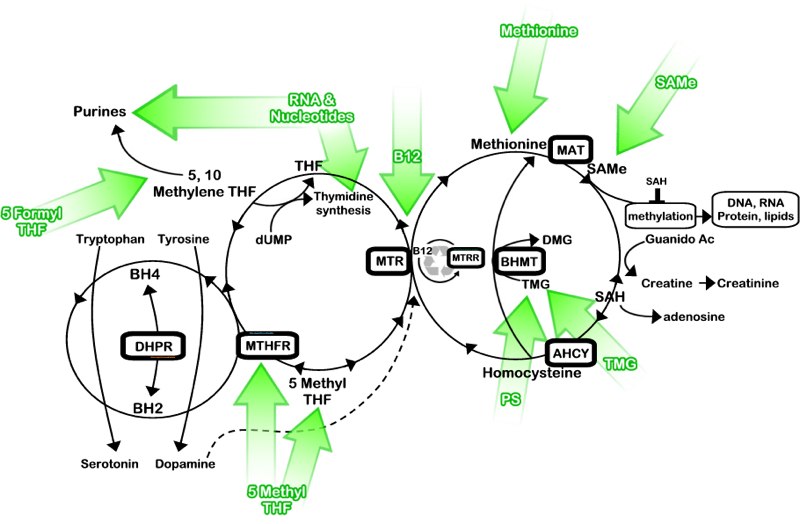
The conversion of MMA to succinic acid requires vitamin B12. The metabolic pathway for MMA is show in the photos below.
Vitamin B12 deficiency impedes this pathway and causes MMA levels to increase. Thus, as water builds up behind a dam, high uMMA levels indicate a vitamin B12 deficiency.
Medical practitioners and Alternative Health Clinics:
Please contact us via telephone or email and we will be pleased to set your facility up as an intake location for this critical test.
Additional shipping fees apply to Hawaii, Alaska, off shore American territories and possessions and to International orders.
uMMA test:
The uMMA test will reveal if the tissue is using B12. The uMMA test is noninvasive (it is a simple urinalysis) and is a much more discrete test than a serum MMA.
The uMMA test is a functional assay. uMMA reflects cobalamin (Vitamin B12) activity at the tissue/cellular level since MMA levels are directly related to a B12-dependent metabolic pathway.
The conversion of MMA to succinic acid requires vitamin B12. The metabolic pathway for MMA is show in the photos below.
Vitamin B12 deficiency impedes this pathway and causes MMA levels to increase. Thus, as water builds up behind a dam, high uMMA levels indicate a vitamin B12 deficiency.
Medical practitioners and Alternative Health Clinics:
Please contact us via telephone or email and we will be pleased to set your facility up as an intake location for this critical test.
Healing Partnerships has been aiding Norman Clinical Laboratories, Inc. in the educational outreach and marketing of the uMMA for several years. It is our goal to see this test as a standard intake test in every hospital, skilled nursing facility, intermediate care facility, drug and alcohol recovery clinic, and group home in America.
Norman Clinical Laboratory, Inc. (NCL) provides a means to test individuals through the mail for cobalamin (vitamin B12 ) deficiency. The test measures methylmalonic acid (MMA) by selected ion monitoring isotope dilution gas chromatography mass spectrometry (GC/MS) in a random spot urine specimen. The MMA value is normalized to urine creatinine to correct for urine dilution. The urinary MMA/creatinine ratio (uMMA) test is more accurate than the blood test as it indicates tissue/cellular B12 deficiency.
This test is often used by physicians wishing to make a conclusive diagnosis of vitamin B12 deficiency with a single test, individuals desiring to be tested by mail from the privacy of their home, and investigators seeking to conduct the most valid research study.
Vitamin B12 deficiency can cause dementia identical to early stage Alzheimer's disease (AD). In addition, vitamin B12 deficiency has been implicated as a risk factor for developing AD. Vitamin B12 deficiency can also cause a wide range of neurologic and/or psychological symptoms, anemia, and is a risk factor for cardiovascular disease. Early detection and treatment usually with vitamin B12 injections can reverse disability.
Strict vegetarians and breast fed infants of vegans are at risk of having B12 deficiency. Vitamin B12 is found only in animal sources such as meat, fish, eggs and milk. Unless a person is a vegetarian, vitamin B12 deficiency is usually caused from malabsorption due to lack of the stomach protein, intrinsic factor, resulting in pernicious anemia. A mild type B12 deficiency is found in some elderly individuals affected with atrophic gastritis. Eating fortified cereals and/or taking multivitamin supplements may eliminate some B12 deficiency in this population 1,2 but yearly uMMA screening is still warranted.
It is important to accurately diagnose vitamin B12 deficiency since treatment may be extensive. For example, individuals with neurologic manifestations, the recommendation is for a B12 injection intramuscular (IM) of 1,000 micrograms daily for 2 weeks, then every two weeks for 6 months, and then monthly for life.3 Some physicians may treat using high amounts of oral B124, intranasal B12 4A, or sublingual B12.5However, adequate response to serious neurologic symptoms to oral therapy has not been conclusively proven.6 Follow up uMMA levels on individuals receiving oral, intranasal B12, or sublingual B12 will assess compliance as well as B12 absorption and assimilation for correction of B12 deficiency at the tissue level.5
Vitamin B12 deficiency can also cause elevated levels of serum homocysteine (Hcys) which have been shown to be a risk factor for strokes, heart attacks and /or blood clots.7
The uMMA test was developed by Eric J. Norman, Ph.D. in collaboration with the late M. Drue Denton, M.D. and co-workers at the Hematology Division of the University of Cincinnati College of Medicine, USA.8,9 This pioneering research continued to:
Norman Clinical Laboratory, Inc. (NCL) provides a means to test individuals through the mail for cobalamin (vitamin B12 ) deficiency. The test measures methylmalonic acid (MMA) by selected ion monitoring isotope dilution gas chromatography mass spectrometry (GC/MS) in a random spot urine specimen. The MMA value is normalized to urine creatinine to correct for urine dilution. The urinary MMA/creatinine ratio (uMMA) test is more accurate than the blood test as it indicates tissue/cellular B12 deficiency.
This test is often used by physicians wishing to make a conclusive diagnosis of vitamin B12 deficiency with a single test, individuals desiring to be tested by mail from the privacy of their home, and investigators seeking to conduct the most valid research study.
Vitamin B12 deficiency can cause dementia identical to early stage Alzheimer's disease (AD). In addition, vitamin B12 deficiency has been implicated as a risk factor for developing AD. Vitamin B12 deficiency can also cause a wide range of neurologic and/or psychological symptoms, anemia, and is a risk factor for cardiovascular disease. Early detection and treatment usually with vitamin B12 injections can reverse disability.
Strict vegetarians and breast fed infants of vegans are at risk of having B12 deficiency. Vitamin B12 is found only in animal sources such as meat, fish, eggs and milk. Unless a person is a vegetarian, vitamin B12 deficiency is usually caused from malabsorption due to lack of the stomach protein, intrinsic factor, resulting in pernicious anemia. A mild type B12 deficiency is found in some elderly individuals affected with atrophic gastritis. Eating fortified cereals and/or taking multivitamin supplements may eliminate some B12 deficiency in this population 1,2 but yearly uMMA screening is still warranted.
It is important to accurately diagnose vitamin B12 deficiency since treatment may be extensive. For example, individuals with neurologic manifestations, the recommendation is for a B12 injection intramuscular (IM) of 1,000 micrograms daily for 2 weeks, then every two weeks for 6 months, and then monthly for life.3 Some physicians may treat using high amounts of oral B124, intranasal B12 4A, or sublingual B12.5However, adequate response to serious neurologic symptoms to oral therapy has not been conclusively proven.6 Follow up uMMA levels on individuals receiving oral, intranasal B12, or sublingual B12 will assess compliance as well as B12 absorption and assimilation for correction of B12 deficiency at the tissue level.5
Vitamin B12 deficiency can also cause elevated levels of serum homocysteine (Hcys) which have been shown to be a risk factor for strokes, heart attacks and /or blood clots.7
The uMMA test was developed by Eric J. Norman, Ph.D. in collaboration with the late M. Drue Denton, M.D. and co-workers at the Hematology Division of the University of Cincinnati College of Medicine, USA.8,9 This pioneering research continued to:
- Identify high prevalence of neurologic disease in vitamin B12 deficient patients without anemia. 9-13
- Identify high prevalence of metabolic B12 deficiency in older populations.9,12-14
- Identify high prevalence of metabolic B12 deficiency in individuals with a normal serum vitamin B12.14-16
- Validate the urinary MMA test as a screening tool for identifying tissue B12 deficiency in older populations.14
- Establish the first commercial laboratory (1985) for measuring normal levels of MMA using gas chromatography mass spectrometry making the assay an available clinical test.
- Establish the first Internet web site (1996) specifically for providing mailing kits and information for the early, non-invasive detection of metabolic vitamin B12 deficiency.